

Introducing Zinda Futures
The Future of Medicine Is Personal...Unless the Data Leaves You Out

Starting a new side to Zinda.
This is the manifesto idea behind Zinda Futures: medicine is changing quickly, but every medical revolution carries the assumptions of the data used to build it.
The concept for the series came out of the recent South asian specific internal AI benchmark we ran at Zinda. We were testing whether AI systems could reason through South Asian clinical risk, and the result took me into a rabbit hole of understanding blind spots.
The benchmark made the core issue impossible to ignore: if the underlying clinical map is miscalibrated, every future tool built on top of it will inherit that miscalibration.
What Happens When Medical AI Sees South Asian Patients?

There is a sentence I have heard too many times in medicine:
So great, once we have built out a refined understanding of the phenotype, how do we solve this?
The question is not only, “What is coming next?”
It should be temporal and intentional: will South Asian biology be included before the future becomes standard of care?
Why?
We are at a unique time in history where the the convergence of technologies in healthcare will accelerate in advances, shifting foundationally, which provides an opportunity to recalibrate South asian medicine from the ground up.
Most of us grew up with a version of medicine built around the disease label.
You have diabetes. You have high cholesterol. You have arthritis. You have coronary disease. You have fatty liver.
That label matters. But it is not the whole story.
The next era of medicine is moving one layer deeper. It will ask a different question:
Which pathway is failing in you?
For one person, the answer may be an inherited gene variant. For another, it may be an enzyme that does not work well, a transporter that changes how a medication is processed, an immune system that is overactivated, a mitochondrial system that cannot keep up, or a tissue environment that cannot repair properly.
That is where medicine is going. From diagnosis to mechanism.
The phrase I keep coming back to is mechanism-calibrated medicine. Or even calibrated medicine.
Not just personalized medicine in the loose consumer sense. Not just concierge care with more labs.
Mechanism-calibrated medicine means using population data, molecular biology, longitudinal measurement, imaging, genetics, bioenergetics, and clinical context together to ask: which mechanism matters in this person, and how should the interpretation be calibrated for the body in front of us?
And for South Asians, this matters more than most people realize.
The old model treated averages
Modern medicine has done incredible things. Vaccines, antibiotics, statins, insulin, surgery, transplantation. We should not pretend the old model failed.
But the old model was built around averages.
Average BMI cutoffs. Average diabetes thresholds. Average cardiovascular risk calculators. Average drug doses. Average trial participants.
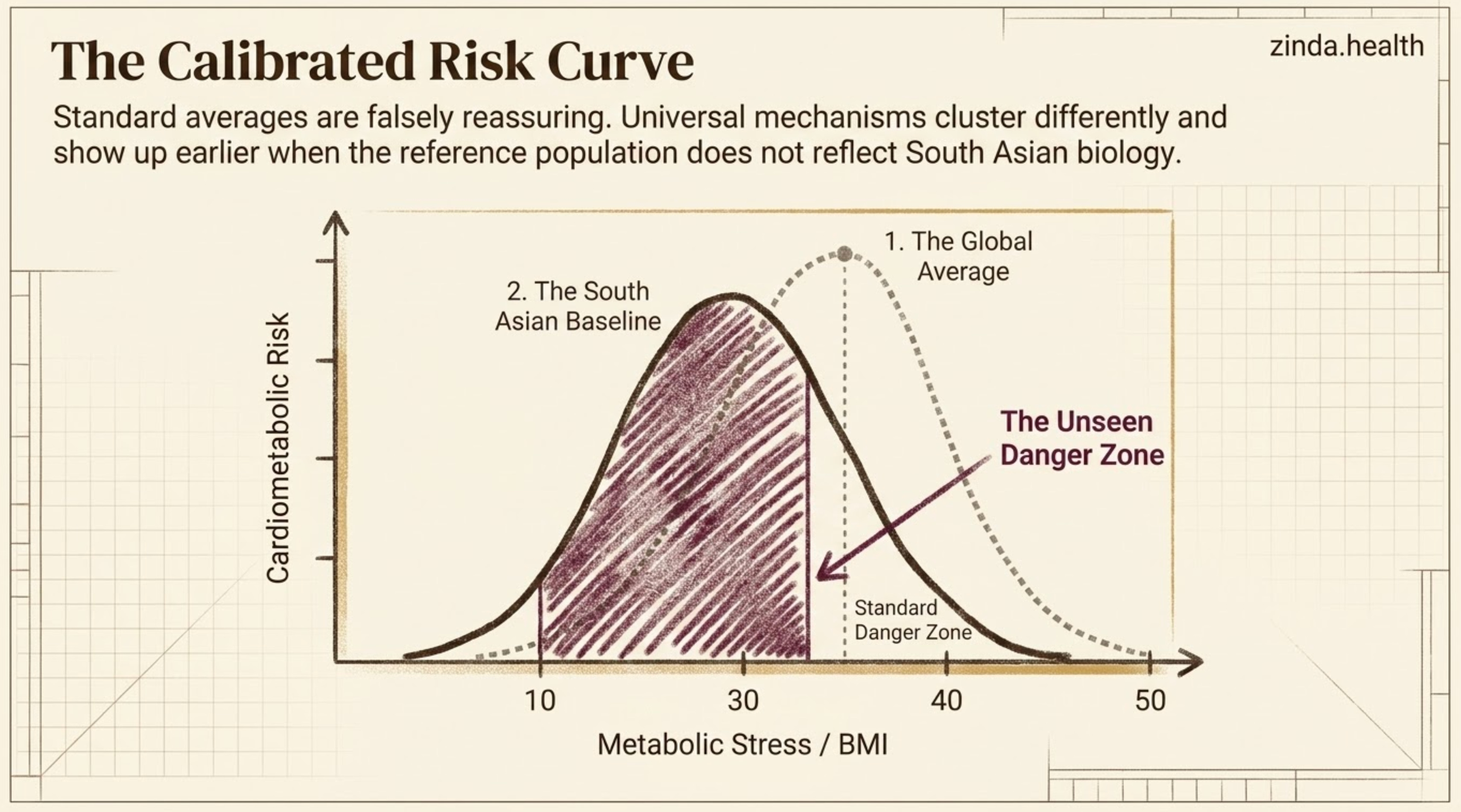
The problem is that South Asians have often lived at the edge of those averages.
We develop insulin resistance at lower BMI. We can carry higher cardiometabolic risk even when standard numbers look “not that bad.” We have different patterns of visceral fat, muscle mass, lipid particles, inflammatory tone, and family-history risk. And in many clinical datasets, we are either underrepresented or grouped into broad categories that blur important differences between Indian, Pakistani, Bangladeshi, Sri Lankan, Nepali, and diaspora populations.
So when medicine becomes more personalized, the question is not just whether the technology gets better.
The question is whether the data finally includes us.
The new model treats pathways
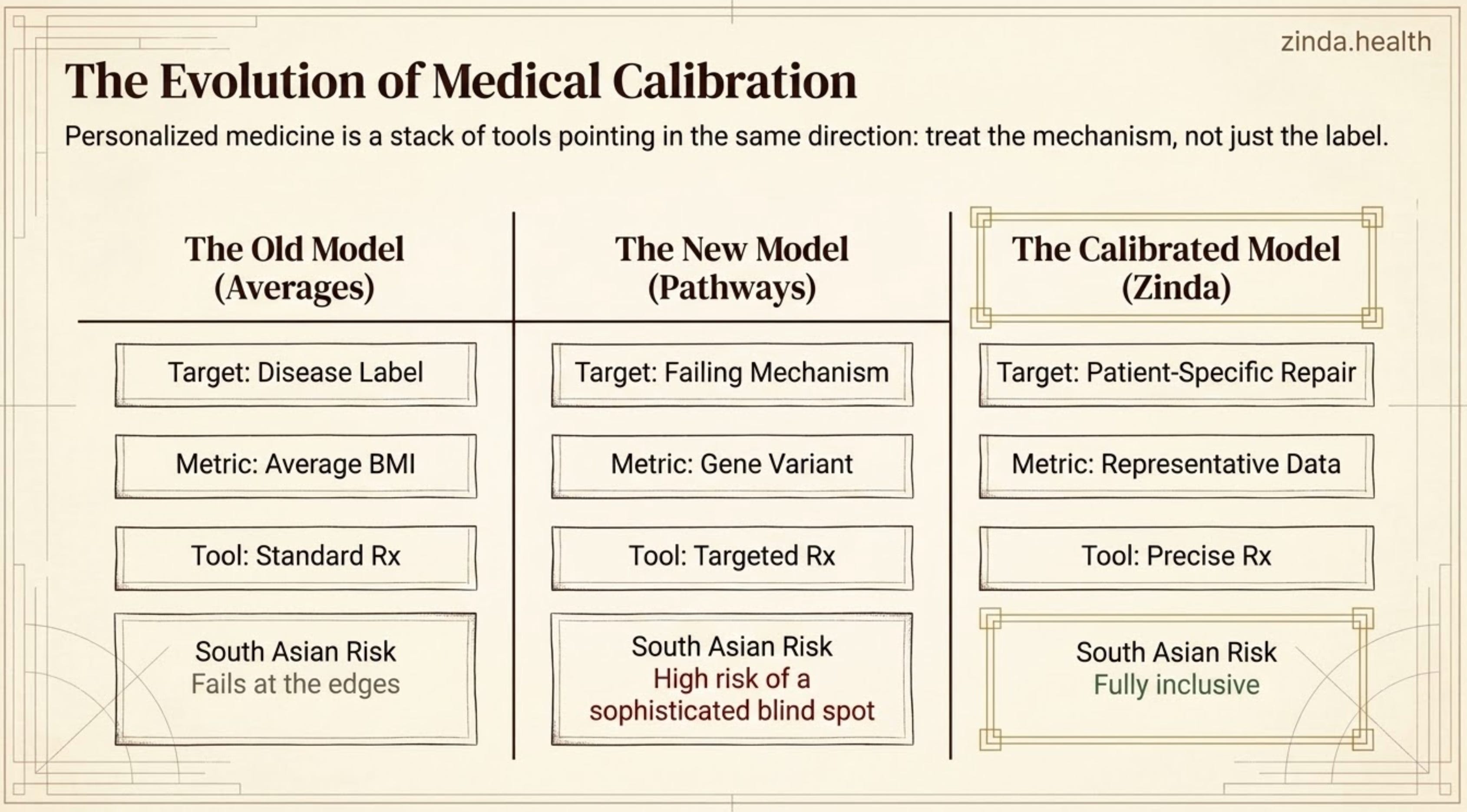
Personalized medicine is not one thing. It is a stack of tools that all point in the same direction: treat the mechanism, not just the label.
That is why mechanism-calibrated medicine may be the better term for what is emerging.
It is not replacing population health. It is layering mechanisms on top of population data. The population tells us the prior probability: who tends to be missed, who develops disease earlier, which pathways cluster together, which thresholds need adjustment. The mechanism tells us what is actually happening inside the person: gene, enzyme, transporter, mitochondrial system, immune pathway, plaque phenotype, tissue niche, repair capacity.
Some examples are already here.
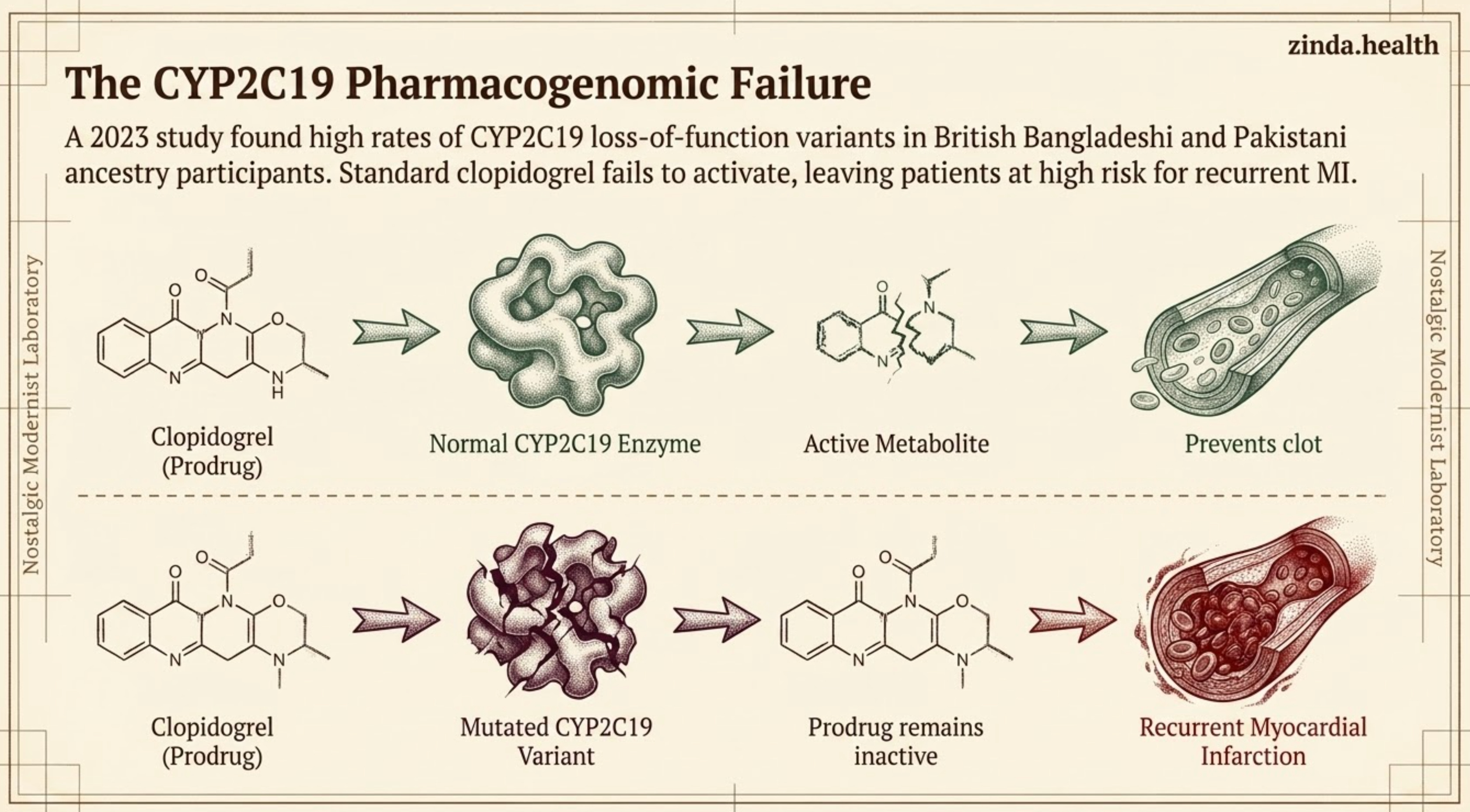
Clopidogrel, or Plavix, has to be activated by the CYP2C19 enzyme. If someone carries certain CYP2C19 loss-of-function variants, the medication may not work the way we expect. That is not a philosophical point. A 2023 JACC: Advances study in British Bangladeshi and Pakistani ancestry participants found a high burden of intermediate and poor CYP2C19 metabolizers, and poor metabolizers prescribed clopidogrel after myocardial infarction had a higher risk of recurrent MI.
Statins are another example. We often talk about statins as if dose is the only variable. But transporter genes such as SLCO1B1 and ABCG2 can affect exposure and tolerability for certain statins. That does not mean South Asians need less prevention. Usually the opposite is true: many need earlier and more aggressive ApoB lowering. But it does mean the path to staying on therapy may need to be smarter.
Lp(a) is another case we’ve spoken about at length on this publication.
Then there are enzyme-targeted treatments: enzyme replacement therapy, chaperone therapy, substrate reduction, mRNA therapies, and gene therapies for conditions where a specific enzyme pathway is broken. Fabry disease is a classic example, but the broader lesson is bigger than rare disease. The more precisely we understand a pathway, the more precisely we can intervene.
This is the pattern: genes, enzymes, receptors, transporters, immune signatures, RNA expression, and tissue repair pathways are becoming clinically actionable.
Some layers are already clinically actionable, like the ones above. Others, like mitochondrial and bioenergetic medicine, are emerging layers that may help explain why risk, repair, and treatment response differ across patients.
Regenerative medicine will be personal too
Regenerative medicine is exciting and something I believe will truly change human health trajectories. Yet, as a consequence of being nascent, it is often described too vaguely. People hear “stem cells” and imagine a universal repair fluid.
That is not how repair works.
A cell therapy or regenerative treatment enters a specific body. That body has a specific immune system, vascular supply, inflammatory state, mitochondrial capacity, glycation burden, microbiome, scar-forming tendency, and genetic background.
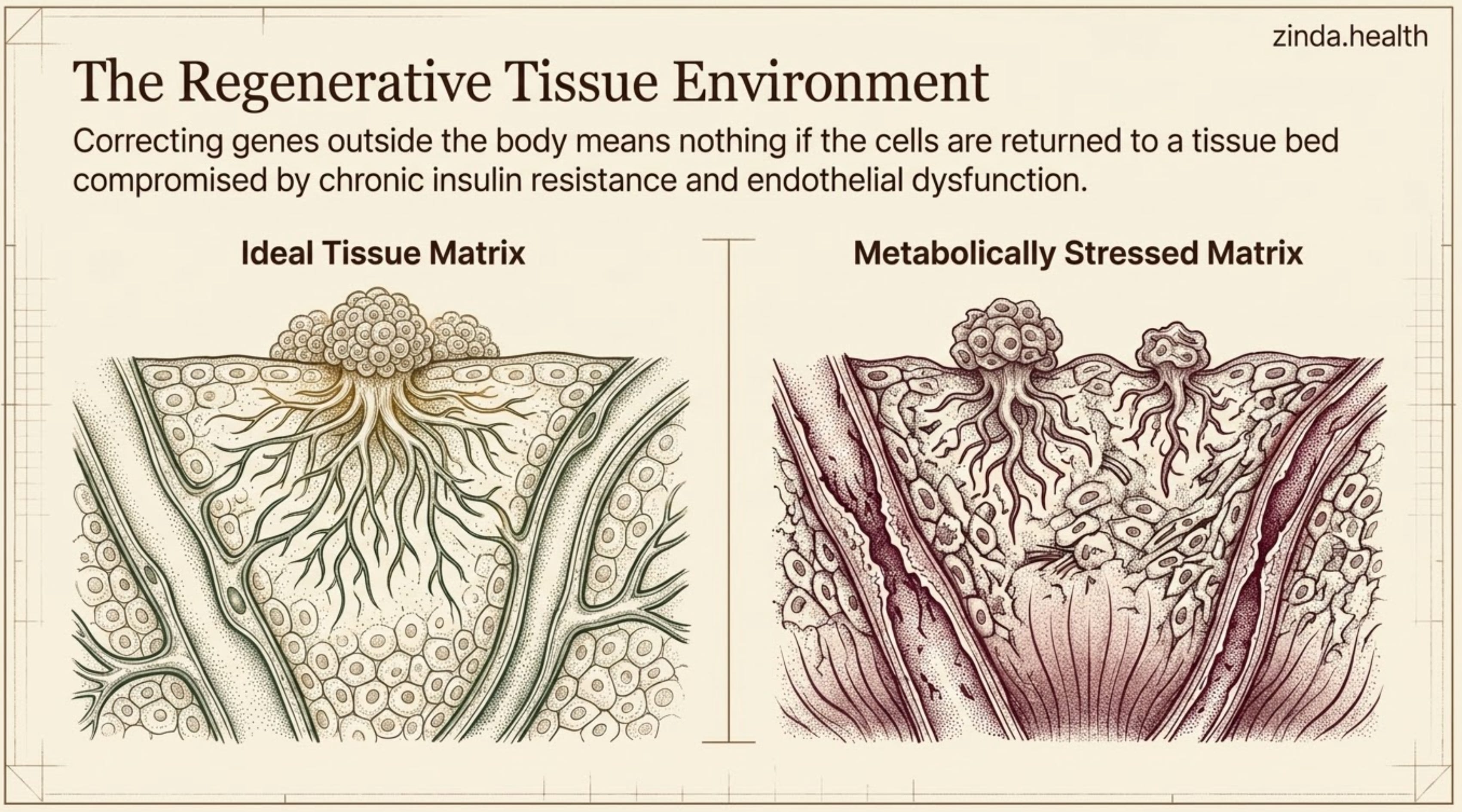
The tissue environment matters.
This is where genetics, metabolic, mitochondria and regenerative medicine start to merge. Induced pluripotent stem cells, or iPSCs, can be made from a patient’s own cells. In theory, those cells can be studied, corrected, engineered, differentiated into a target cell type, and potentially returned to the patient. This is still an evolving field, and safety matters: tumor risk, immune reaction, off-target editing, durability, and whether the new tissue behaves normally once it is back inside the body. All these must take into account the environment.
Regeneration will not just be “replace the tissue.” It will be: understand the patient’s repair biology, then decide what kind of repair is actually possible.
For South Asians, that question becomes even more important.
If a person has chronic insulin resistance, endothelial dysfunction, visceral adiposity, low-grade inflammation, vitamin D or B12 issues, mitochondrial stress, or accelerated vascular aging, those factors may affect how well tissue repair works.
Though I will premise this by saying we should be careful in specificying too much towards one phenotype as we do not yet have enough data, let alone South Asian-specific regenerative medicine data, to make sweeping claims.
But that is exactly the point.
If regenerative medicine is going to become personal, South Asian biology cannot be an afterthought.
The risk is a more sophisticated blind spot
There is a comforting story people tell about precision medicine: once medicine becomes genetic and molecular, it will automatically become fair.
I do not think that is necessarily the case.
We have seen this before. More technical medicine does not automatically become more equitable. Polygenic scores can fail when built on European-ancestry data. Pharmacogenomic algorithms can miss ancestry-specific variants. Pulse oximeters looked objective until they missed hypoxemia more often in darker skin. Kidney and lung equations used race as calibration and sometimes turned difference into delayed diagnosis. The lesson is simple: precision without representative data is not precision for everyone.
Even an AI model trained on incomplete clinical data can sound precise while being wrong for the person in front of it.
We have already seen the simpler version of this problem.
South Asian patients are told their BMI is fine when their visceral fat is not. Their LDL is “acceptable” when their ApoB or Lp(a) says otherwise. Their calcium score is reassuring when the question is soft plaque. Their glucose is normal until the post-meal spike appears. Their family history is noted but not modeled deeply enough.
The future can repeat the same mistake, just at a molecular level.
That is what we have to avoid.
What Zinda Futures is for
This is why Zinda Futures exists.
The AI benchmark was the trigger, but the lesson applies beyond AI.
Not to predict every new technology.
Not to chase hype.
But to ask a practical question before the future becomes standard of care:
What does South Asian health need to build now so the next generation of medicine is calibrated correctly from the beginning?
That means each future-facing question has to become a build agenda.
If medicine is moving toward pharmacogenomics, we need South Asian pharmacogenomic maps that clinicians can actually use.
If prevention is moving from LDL-C alone toward ApoB, Lp(a), and plaque imaging, we need South Asian-specific decision pathways for when the usual numbers are falsely reassuring.
If risk prediction is moving toward polygenic scores and AI models, we need to know which datasets trained them, which ancestry groups validated them, and where the scores fail.
If regenerative medicine is moving toward patient-specific repair biology, we need to study the South Asian tissue environment: insulin resistance, endothelial dysfunction, inflammation, mitochondrial stress, glycation burden, vitamin status, and the biology that determines whether repair works.
So Zinda Futures has a simple job:
name where medicine is going
identify the South Asian gap before it hardens into a standard
explain the mechanism behind the gap
turn the gap into something Zinda can measure, publish, build, or advocate for
How the Zinda framework compounds
The important thing is that Zinda Futures does not sit on top of vibes (sorry Andrej, I had to).