

The Vanishing Engine, Part II
The intervention architecture for South Asian muscle

This article is for educational and informational purposes only and does not constitute medical advice. The information presented reflects current research and should not replace consultation with qualified healthcare providers. Individual treatment decisions, particularly regarding prescription medications, peptides, and supplements, should be made in partnership with your physician based on your specific circumstances. Additionally, I do not sell any of these supplements or stand to gain from endorsing them.
Goal remains the same…South Asian health optimization.
In Part I, we mapped the architecture of South Asian sarcopenia: the fetal programming that sacrifices muscle for fat, the dissociated mitochondria running hot, and the hormonal axes that compound it all. We established that muscle is not merely mechanical tissue but a metabolic organ.
Losing muscle is organ failure. And we are losing this battle.
The question now is what to do about it.
What follows is a comprehensive structure on how we can approach it.
The Intervention Architecture
If the South Asian body is built for conservation, storing fat, minimizing muscle, rationing energy, then the intervention strategy must be designed to override these defaults. It must be aggressive, multimodal, and sustained.
Consider how we approach dyslipidemia in South Asians which we touched a bit on Chai Shots earlier this month. We do not tell a patient with Lp(a) of 150 nmol/L to “just eat better.”
We recognize that the genetic architecture is set, that lifestyle alone, while necessary, cannot overcome the magnitude of the inherited risk.
We layer interventions: diet modification, exercise, and pharmacology working in concert. We monitor biomarkers. We titrate aggressively.
Sarcopenia in South Asians demands the same approach. The upregulated myostatin signaling suppressing hypertrophy, the developmental programming favoring fat over muscle, the mitochondria running hot but failing to clear lipids, these are not lifestyle problems with lifestyle solutions. They are genetic headwinds requiring metabolic intervention.
The current clinical approach, ”lift weights, eat protein,” is analogous to telling someone with familial hypercholesterolemia to reduce saturated fat. It is not wrong. It is woefully insufficient.
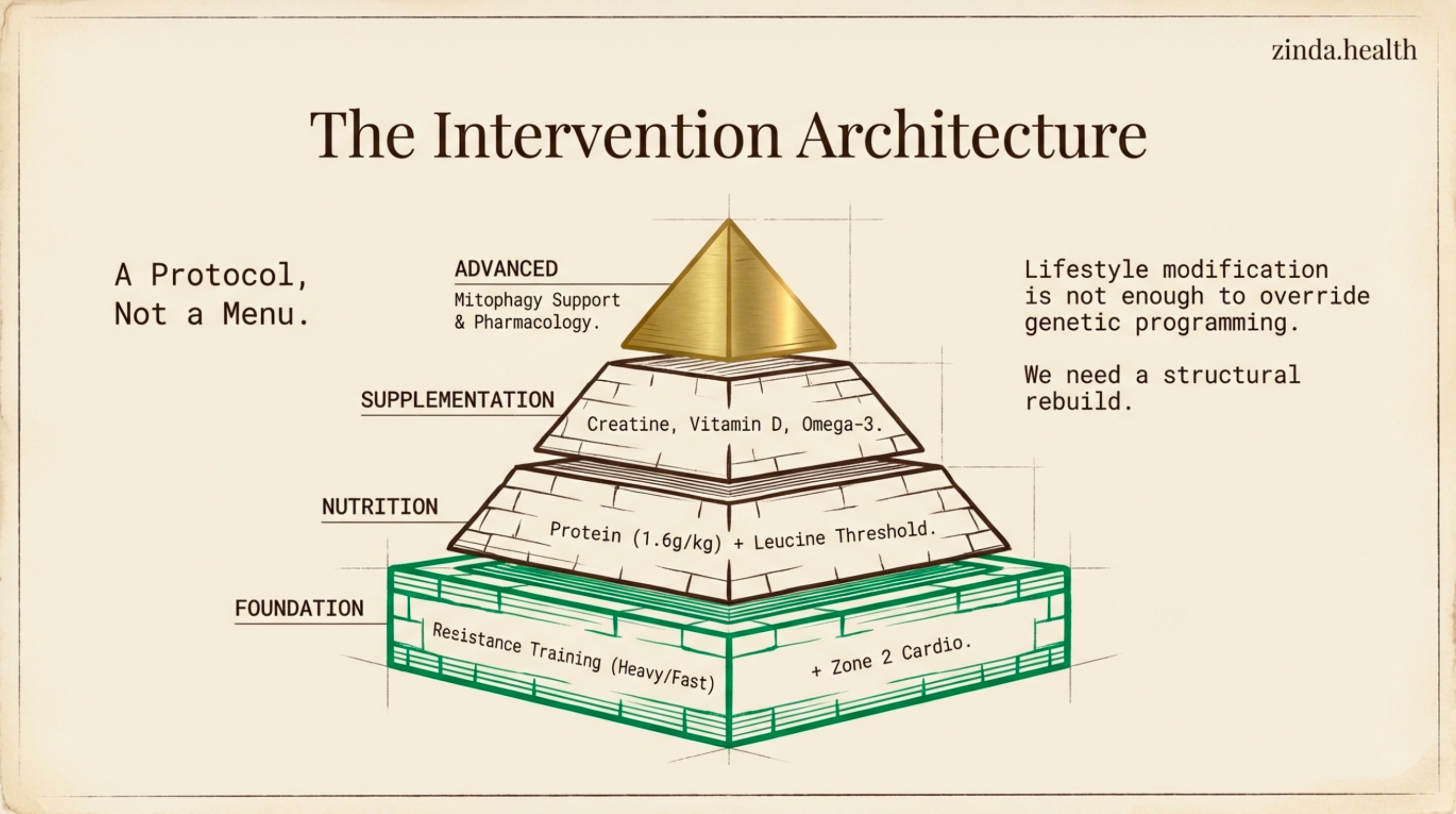
What follows is a comprehensive architecture built on three pillars:
exercise programming (not generic, but South Asian-specific)
peri-exercise optimization (what you do before and after matters as much as the training itself)
pharmacological support (the interventions that address what lifestyle cannot).
This is not a menu of options. It is a layered framework that begins with non-negotiable foundations and builds upward toward targeted enhancement.
Foundation Layer: South Asian-Specific Exercise Programming
1. Volume and Frequency
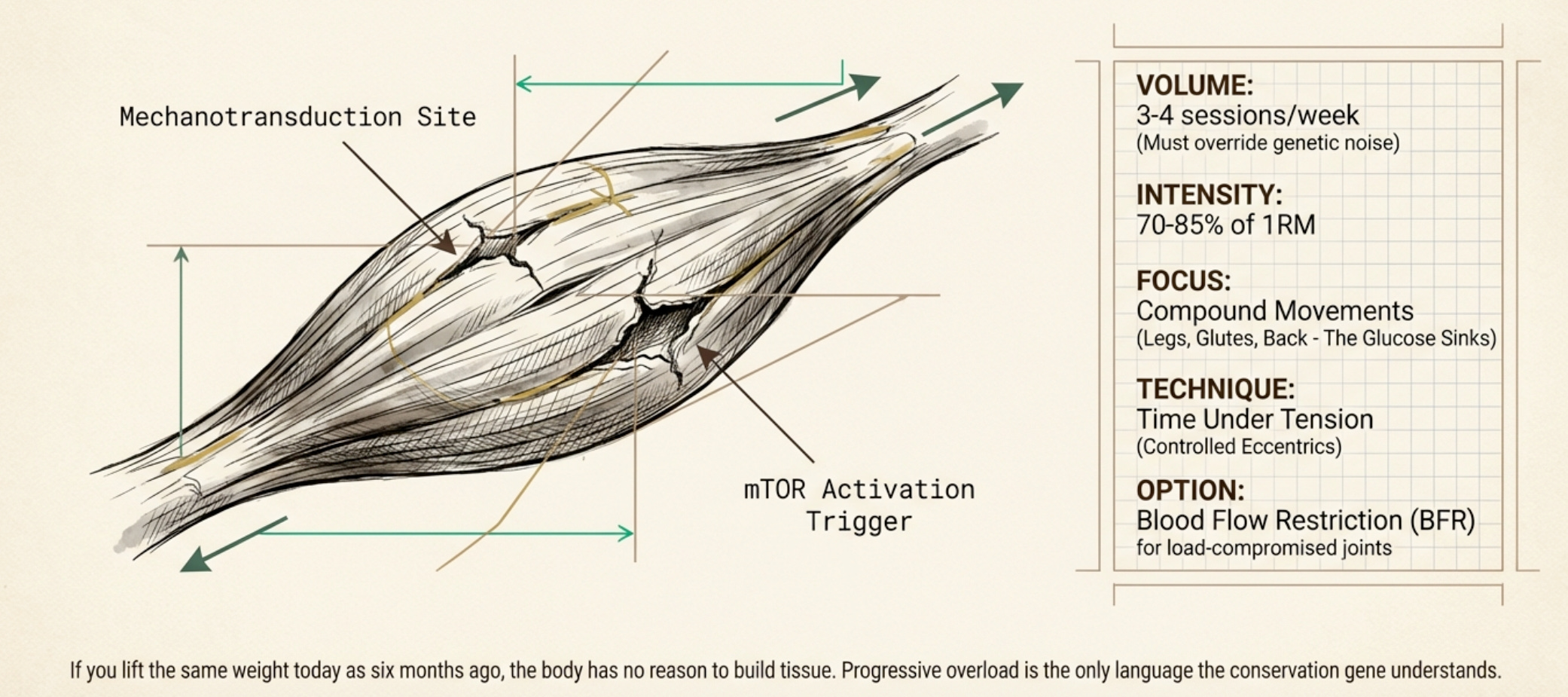
Meta-analyses show resistance training at 70-85% of one-repetition maximum produces the greatest gains. However, for South Asians fighting myostatin-mediated suppression, the volume must exceed generic guidelines.
Target: 3 - 4 sessions/week.
The Reasoning: The signal must be louder to overcome the genetic noise. If you train infrequently, the conservation-programmed body simply reverts to baseline. You must present a constant demand that makes muscle maintenance a survival priority.
2. Compound Movements First
The largest glucose sinks in the body are the legs, glutes, and back. Squats, deadlifts, rows, and presses help build this as a core.
The Reasoning: These muscles, when developed, create the metabolic runway we lack. Isolation exercises (like bicep curls) have their place, but they cannot substitute for the systemic anabolic signal that compound movements generate.
3. Time Under Tension & Eccentrics
Moving weight is not enough. The muscle must experience sustained mechanical tension to trigger the mTOR pathway.
The Tactic: Controlled eccentrics (lowering phase), pauses at the bottom, and deliberate tempo.
The Reasoning: Rushing through sets with momentum defeats the purpose. You must mechanically stress the tissue to signal to a conservation-programmed body: this expensive tissue is needed for survival.
4. Velocity Training (The Spark Plug)
Sarcopenia begins with motor neuron death, specifically the fast-twitch Type II neurons. If you never ask them to fire, they atrophy. Asians usually have significantly less Type II (fast-twitch) muscle fiber density compared to other populations..
The Tactic: Move weights fast. The concentric phase (lifting) should be explosive. Consider “velocity days” with lighter loads (50-60% 1RM) moved with maximum speed.
The Reasoning: Traditional “slow and controlled” lifting builds tension but misses the neural component. Explosive movement keeps the “spark plugs” (motor neurons) firing, preventing the neural disconnect that precedes muscle loss.
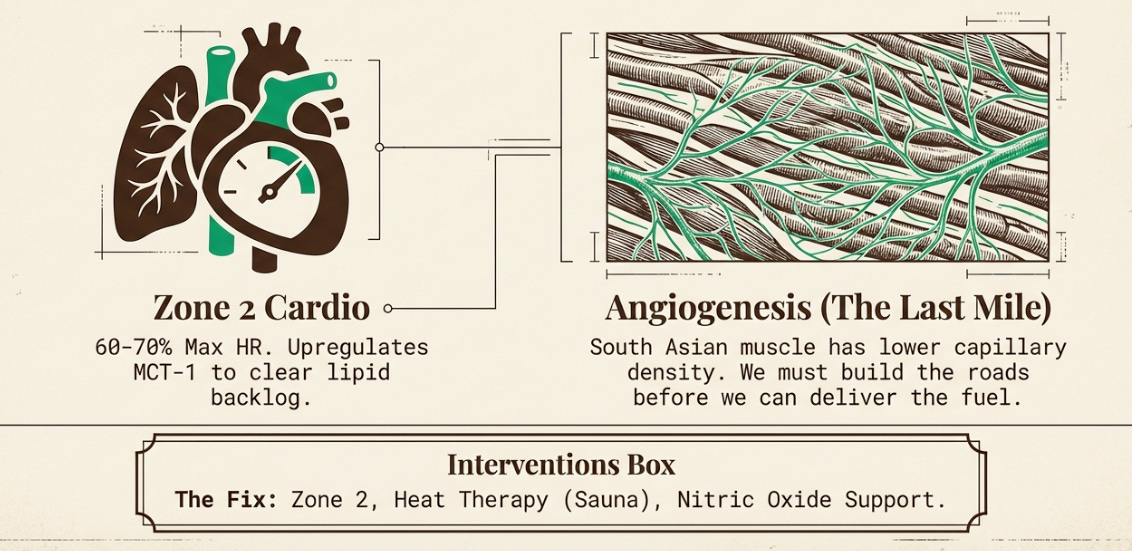
5. Capillary Density: The Last Mile
South Asian muscle often shows lower capillary density. You can flood the bloodstream with nutrients, but if the “last mile” infrastructure is sparse, the muscle starves.
Intervention: Heat therapy (Sauna: 15-20 mins at 170-190°F, 3-4x weekly).
The Reasoning: We have discussed the engine (mitochondria) and the fuel (lipid overflow), but not the road. Sauna use is one of the few interventions that stimulates angiogenesis (new blood vessel growth) independent of mechanical load, building the infrastructure for future training.
This reinforces the nitric oxide interventions discussed below, citrulline and beetroot are not merely for “the pump.” They are for vascular recruitment, opening collateral pathways to reach under-perfused tissue.
Additionally, heat therapy (sauna, 15-20 minutes at 170-190°F, 3-4 times weekly) is one of the few interventions that stimulates angiogenesis, the growth of new capillaries, independent of mechanical load. For the sarcopenic patient who cannot yet train intensely, sauna builds the infrastructure that will eventually support training.
6. Zone 2 for Metabolic Flexibility
By far my favorite…because it rewards patience and consistency. And I want to spend some time on the nuances here as Zone 2 spans a broad definition.
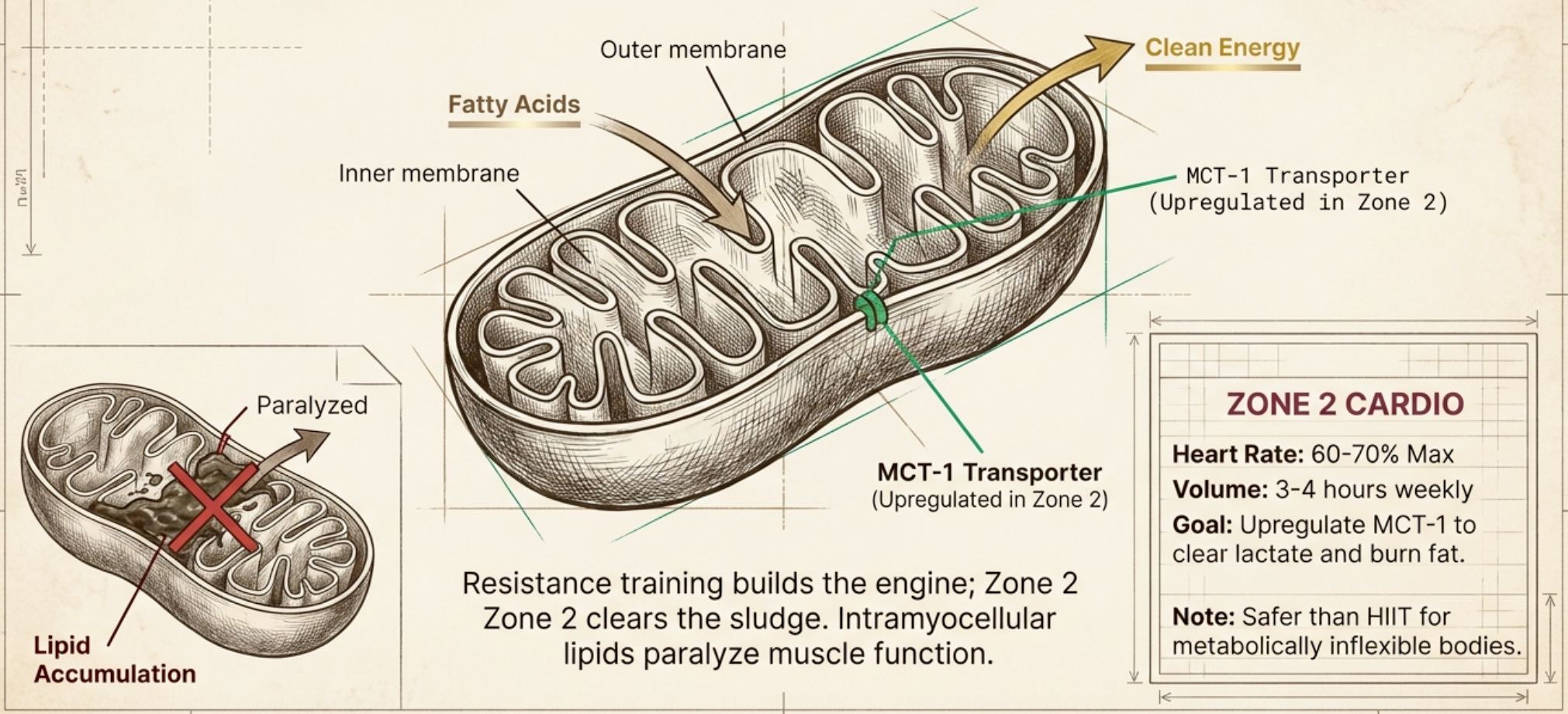
Resistance training alone does not clear the intramyocellular lipid trap. For that, you need aerobic work that preferentially burns fat.
Zone 2 cardio (heart rate 60-70% of maximum, conversational pace, 3-4 hours weekly) remains the foundation for this population. Lower baseline muscle mass and metabolic dysfunction make high-intensity work riskier, Zone 2 offers benefit without the same injury risk or stress load. More importantly, Zone 2 specifically trains fat oxidation pathways and is the only intensity that that upregulates MCT-1 transporters, the machinery that clears lactate. Since metabolically inflexible individuals often run with elevated baseline lactate, Zone 2 addresses this dysfunction directly in a way HIIT cannot. As capacity develops, higher-intensity work can be layered in.
The training stimulus requires nutritional support. Protein intake of 1.6-2.0 g/kg/day of ideal body weight, far higher than the 0.8 g/kg RDA designed for sedentary populations, is the threshold for supporting muscle protein synthesis in a body fighting innate headwinds geneticall. The lower recommendations (1.0-1.2 g/kg) are insufficient when starting from sarcopenic baseline.
Critical to understand: older or insulin-resistant muscle becomes “deaf” to protein signals. You need to exceed a threshold to trigger growth. Leucine, the amino acid that most potently activates the mTOR pathway governing muscle growth, must reach approximately 3.0g per meal to reliably stimulate muscle protein synthesis.
Here is the math based on traditional South Asian diets to provide sufficient protein for muscle building:
Food Source Amount Needed for 3g Leucine Whey protein isolate 1 scoop (25g) Chicken breast 120g (one palm-sized portion) Paneer 200g Greek yogurt 400g Dal (lentils) ~2.5 cups thick / ~9 bowls typical Rice + dal combined Still insufficient without fortification
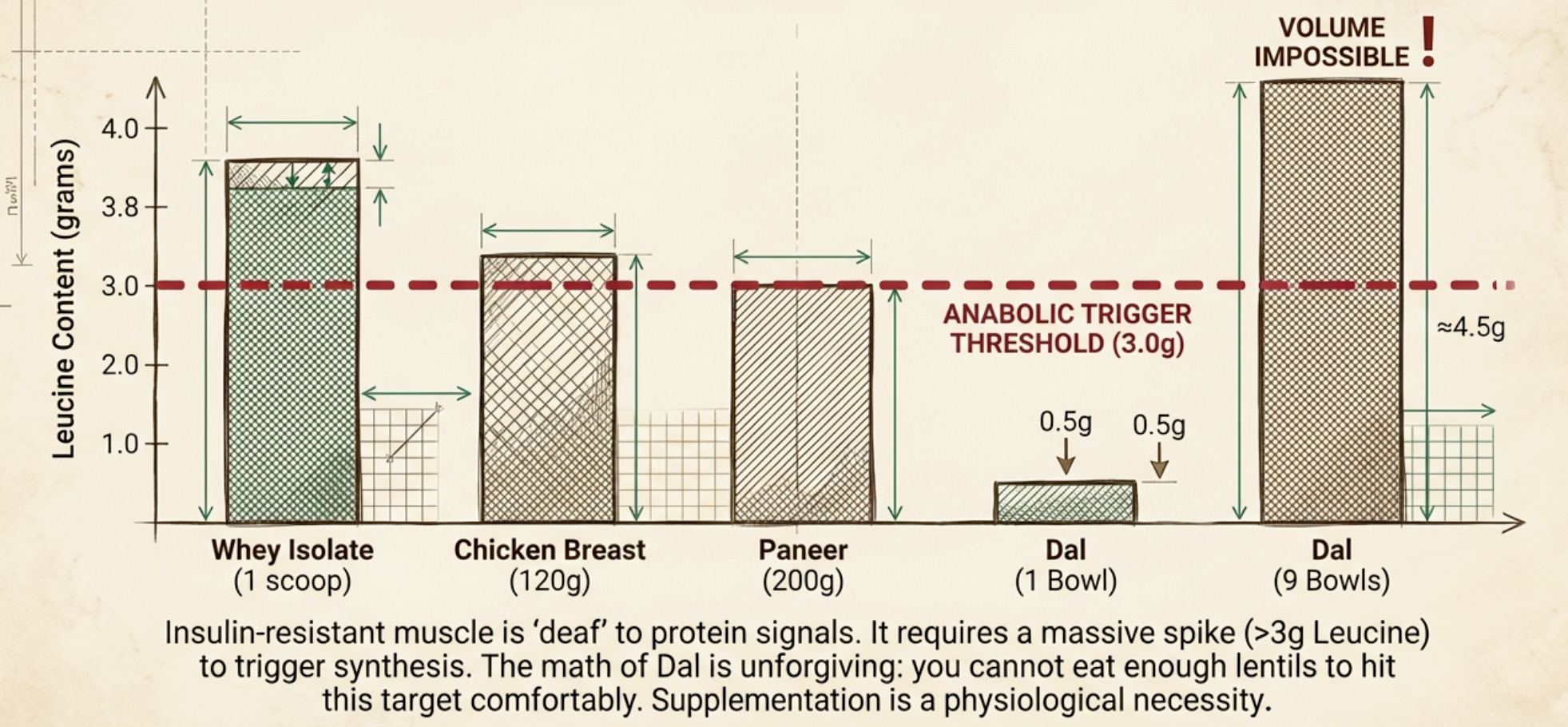
The reality is that atypical bowl of dal contains roughly 0.5g of leucine which is not nearly enough. To hit the leucine threshold from dal alone, you would need to eat over 2.5 cups of thick lentils or nearly 9 bowls of typical homemade dal (almost a full cooker worth!!) in a single sitting. This is not a cultural judgment; it is a mathematical reality. For the vegetarian South Asians, supplementation is a necessity.
This is where cultural dietary patterns often collide with physiological need. Plant-based South Asian diets can provide adequate protein, but they require intention, combining rice with dal, emphasizing paneer and yogurt, adding whey or EAAs to meals. The casual vegetarianism that many families practice is not automatically sufficient for someone trying to build metabolic reserve.
