There is a particular kind of relief that comes with a calcium score of zero.
You book the scan, lie still for a few minutes, and a number comes back: 0.
For many people, that result is genuinely reassuring.
But for South Asians, the deeper question is whether a zero calcium score sees the whole coronary-risk story, especially when family history, symptoms, diabetes, ApoB, Lp(a), or insulin resistance are already raising the signal.
We now have technology to provide nuance in a way never previously available.
This is the kind of question Zinda Futures is built for.
Medicine is moving from simple risk markers toward richer imaging, AI-assisted plaque quantification, and more mechanism-aware prevention. That could be a major advance, especilaly if the tools are calibrated to the biology of the people using them.
For South Asians, calcium scoring can be useful yet still incomplete. A single reassuring number can become the end of the conversation while the biology is still moving underneath it.
A CAC score of zero is one of the strongest negative risk markers we have in preventive cardiology. It can help avoid unnecessary medication in the right person. It can calm down a borderline risk conversation. It is quick, relatively inexpensive, and widely available.
For South Asians, that result should sometimes lead to a second question, because CAC answers a narrower question than many people realize.
A calcium score asks how much plaque has hardened. It is less direct at answering how much plaque is actually there.
And that distinction may matter a lot for us.
What CAC Actually Measures
Coronary artery calcium scoring measures calcified plaque in the coronary arteries. It is looking for the hardened, mineralized footprint of atherosclerosis. When that footprint is large, risk rises. When it is absent, risk is usually lower.
That is why CAC has become so useful in primary prevention. In someone with borderline or intermediate risk, a CAC score can help decide whether to start or intensify preventive therapy. The 2019 ACC/AHA prevention guideline explicitly lists South Asian ancestry as a risk-enhancing factor and supports CAC testing when risk remains uncertain after the usual calculation.
The same guideline also makes the important point that the absence of CAC does not rule out non-calcified plaque.
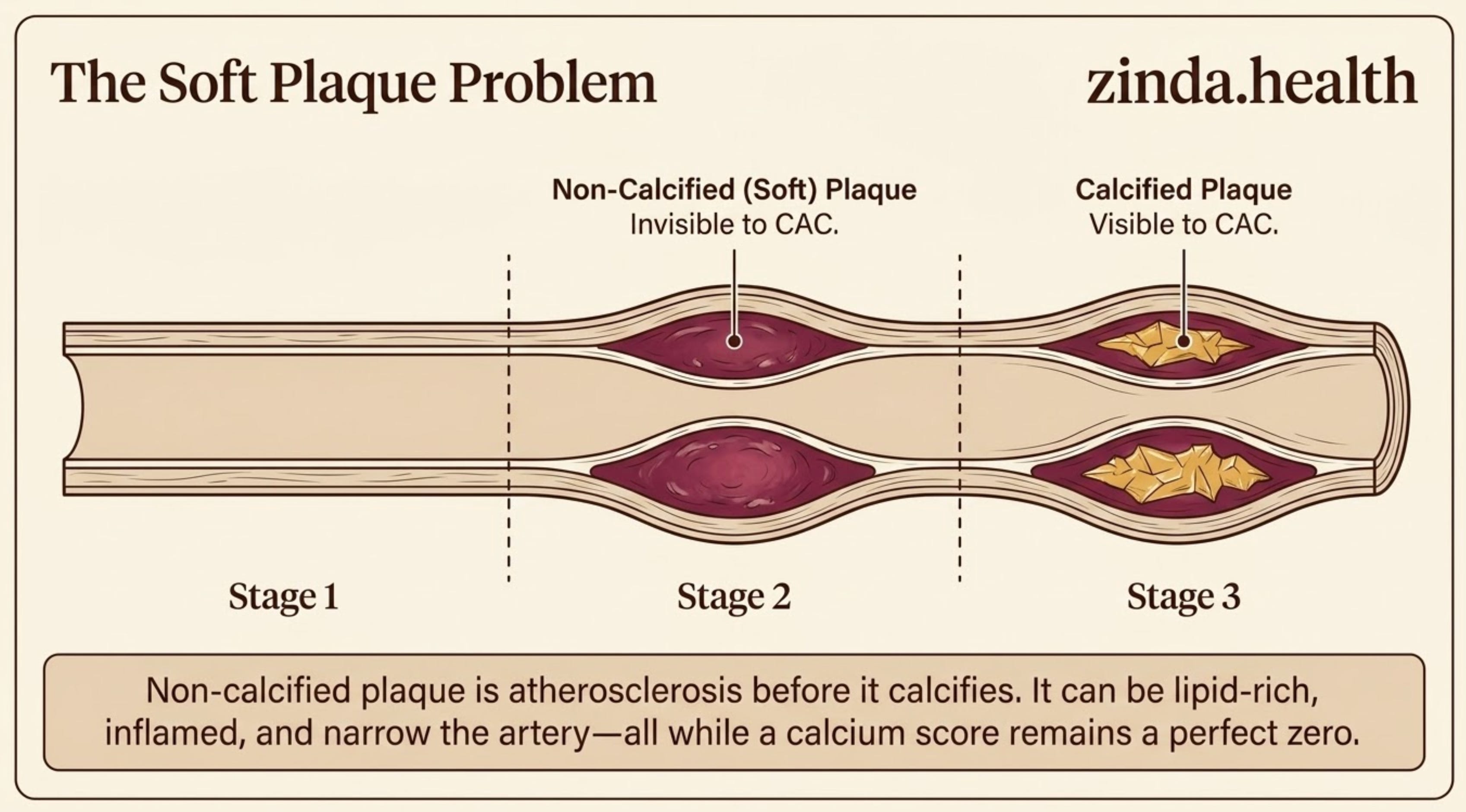
That sentence is easy to skip, but it carries the whole argument. Non-calcified plaque is atherosclerosis before it has calcified. It can be lipid-rich, inflamed, narrowing the artery, and still invisible to a calcium score.
A zero calcium score means the scan did not see calcified plaque. The artery wall may still deserve attention when the clinical story is concerning.
For many low-risk, asymptomatic patients, that nuance may not change much. CAC=0 is still a good sign.
In a South Asian patient with chest pain or premature family history, diabetes or insulin resistance, high ApoB, high Lp(a), central adiposity, or a story that just does not fit the number, that nuance becomes the whole point.
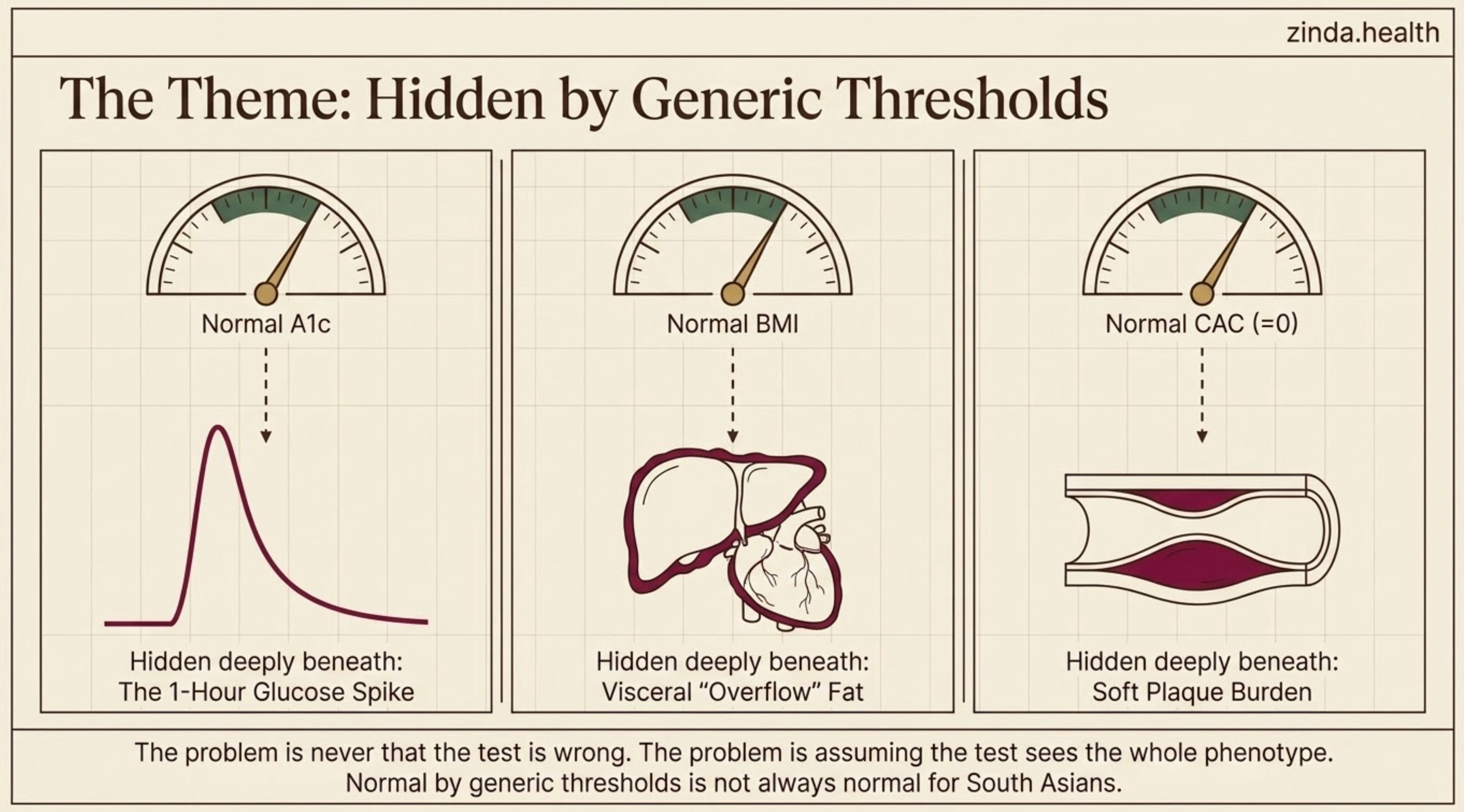
We have seen this pattern before in other parts of the Zinda framework. In The Spike Before the Diagnosis, the A1c can look normal while the first-hour glucose curve is already abnormal. In The Overflow Tank, BMI can look normal while fat is sitting in the liver, pancreas, muscle, and around the heart. In Miscalibrated Lipids, a standard lipid panel can look acceptable while ApoB, Lp(a), and ancestry-specific lipid architecture tell a different story.
The theme is the same:
The danger is assuming one test sees the whole phenotype.
The soft plaque problem
South Asians tend to develop cardiovascular disease earlier, often at lower BMI, often with diabetes or insulin resistance arriving sooner than expected, and often with risk calculators that underestimate what is happening inside the body.
The plaque phenotype may be different too.
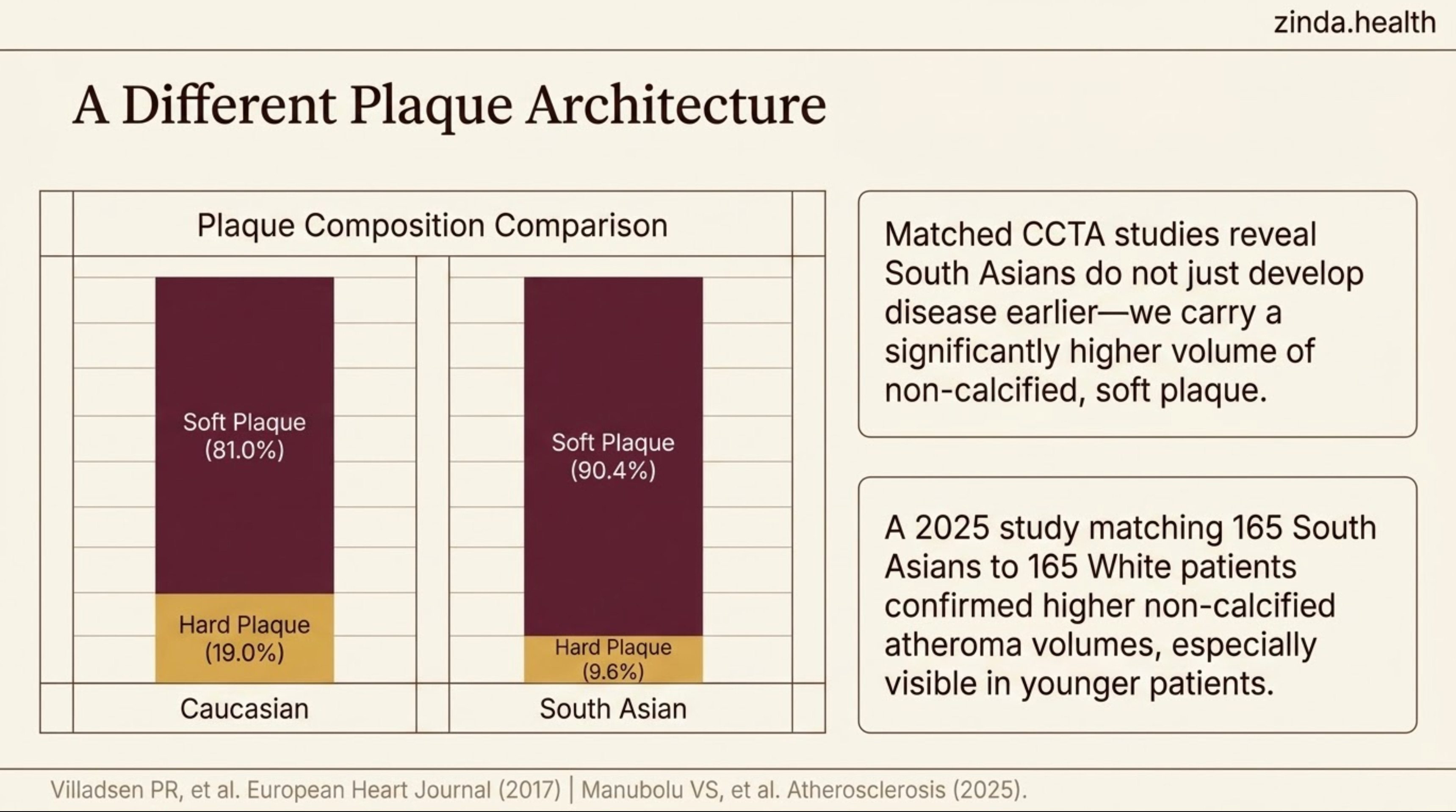
A 2017 study in European Heart Journal – Cardiovascular Imaging compared 543 South Asian patients and 420 Caucasian patients with stable chest pain who underwent coronary CT angiography. South Asian patients were younger and had much higher diabetes prevalence. After adjustment, there was no major difference in total plaque burden or stenosis severity.
But the composition differed.
Among patients with atherosclerotic plaque, the proportion that was non-calcified was higher in South Asians: about 90.4% compared with 81.0% in Caucasian patients.
That is the key signal. Plaque type differed.
A newer 2025 matched CCTA study pushed this further. Researchers matched 165 South Asian patients to 165 non-Hispanic White patients by age, sex, BMI, and diabetes status. South Asians had higher total plaque percent atheroma volume, higher non-calcified plaque percent atheroma volume, and higher calcified plaque percent atheroma volume. The differences were especially visible in younger patients.
So when we say South Asians may carry more soft plaque, the claim is grounded in CCTA-based evidence.
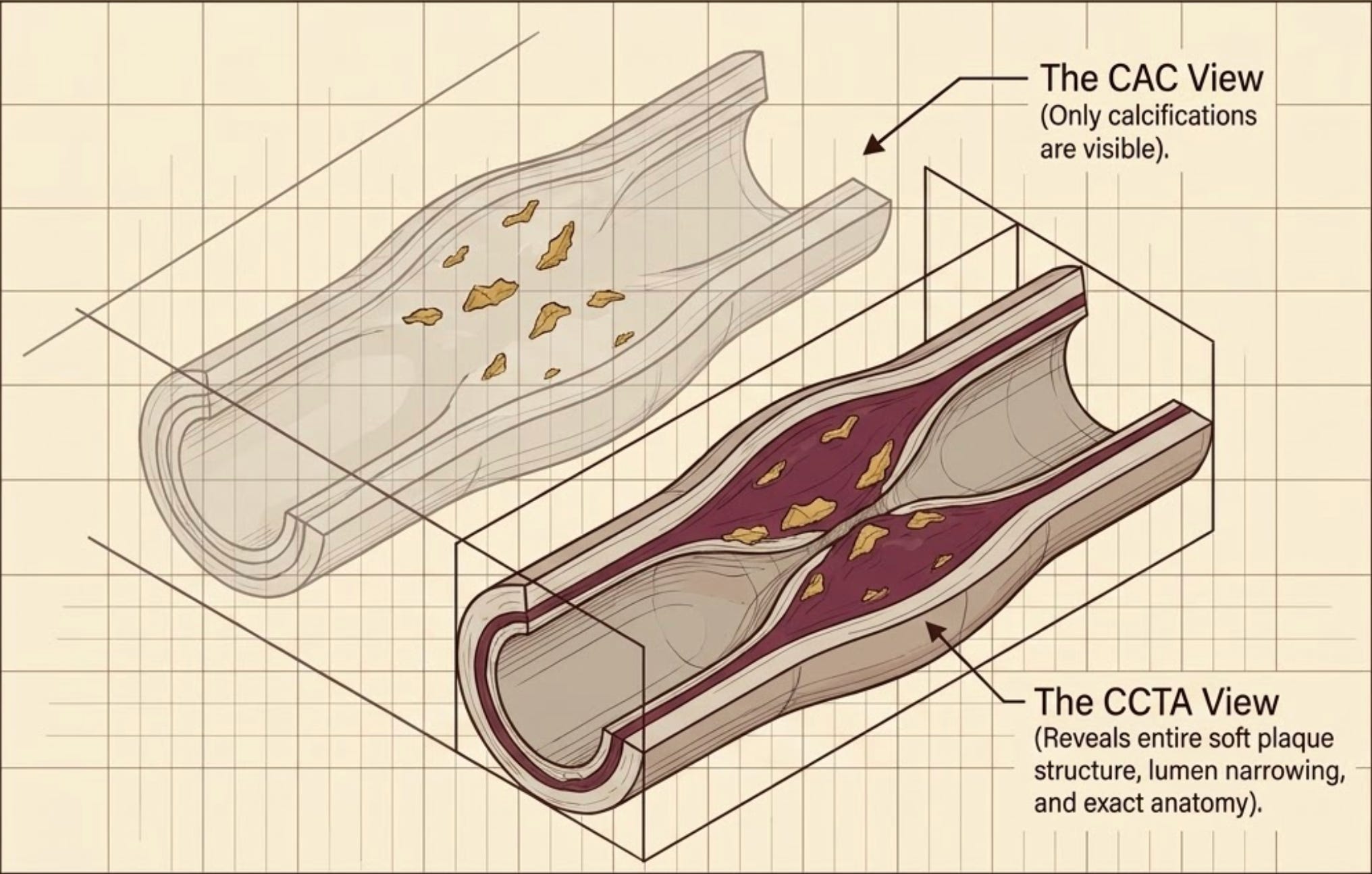
This matters because CAC sees calcium, while CCTA can directly evaluate non-calcified plaque.
The Pakistani zero-CAC study that should make us pause
The cleanest patient-facing example comes from Pakistan.
In a 2024 Global Heart study, Shams and colleagues looked at 534 symptomatic patients of South Asian descent who had a zero Agatston calcium score and underwent CT coronary angiography.
These were symptomatic patients being evaluated for angina-like symptoms or angina equivalents.
The findings are exactly the kind of nuance we need:
28.8% had non-calcified, or soft, coronary plaque of some degree.
5.8% had obstructive coronary artery disease greater than 50%.
Despite that, CAC=0 still carried a favorable long-term prognosis in the cohort.
That last point matters. The study made CAC=0 more precise:
CAC=0 can still be prognostically reassuring while failing to mean “no plaque.”
That is the conversation South Asian patients deserve: reassurance with precision.
It gave us more data for calibration rather than generalization.
If you are asymptomatic and low-risk, CAC=0 may be enough. If you are symptomatic, high-risk, or carrying a family history that makes everyone in the room uneasy, CAC=0 should leave room for another question.
What CCTA adds
Coronary CT angiography asks a different set of questions.
CAC asks whether plaque has calcified.
CCTA can show whether plaque is present at all. It can show where it sits, whether it narrows the artery, whether it is calcified or non-calcified, and whether there are features that make it more concerning.
That is why the 2021 AHA/ACC chest pain guideline gives CCTA a major role in evaluating intermediate-risk patients with acute or stable chest pain and no known coronary artery disease. In stable chest pain patients at intermediate-high risk, CCTA is effective for diagnosis, risk stratification, and guiding treatment decisions.
This is guideline-supported cardiology when the clinical context fits.
Where it becomes especially interesting for South Asians is the plaque-phenotype layer.
If our risk is partly driven by non-calcified plaque, the imaging test that sees non-calcified plaque may be the more biologically appropriate test in selected patients.
Again, selected patients.
A good pathway does not put every South Asian adult through a CCTA scanner. It reserves the stronger lens for the moments when CAC is being asked to answer a question it cannot fully answer.
Where Cleerly and HeartFlow fit
This is where the newer tools become important.
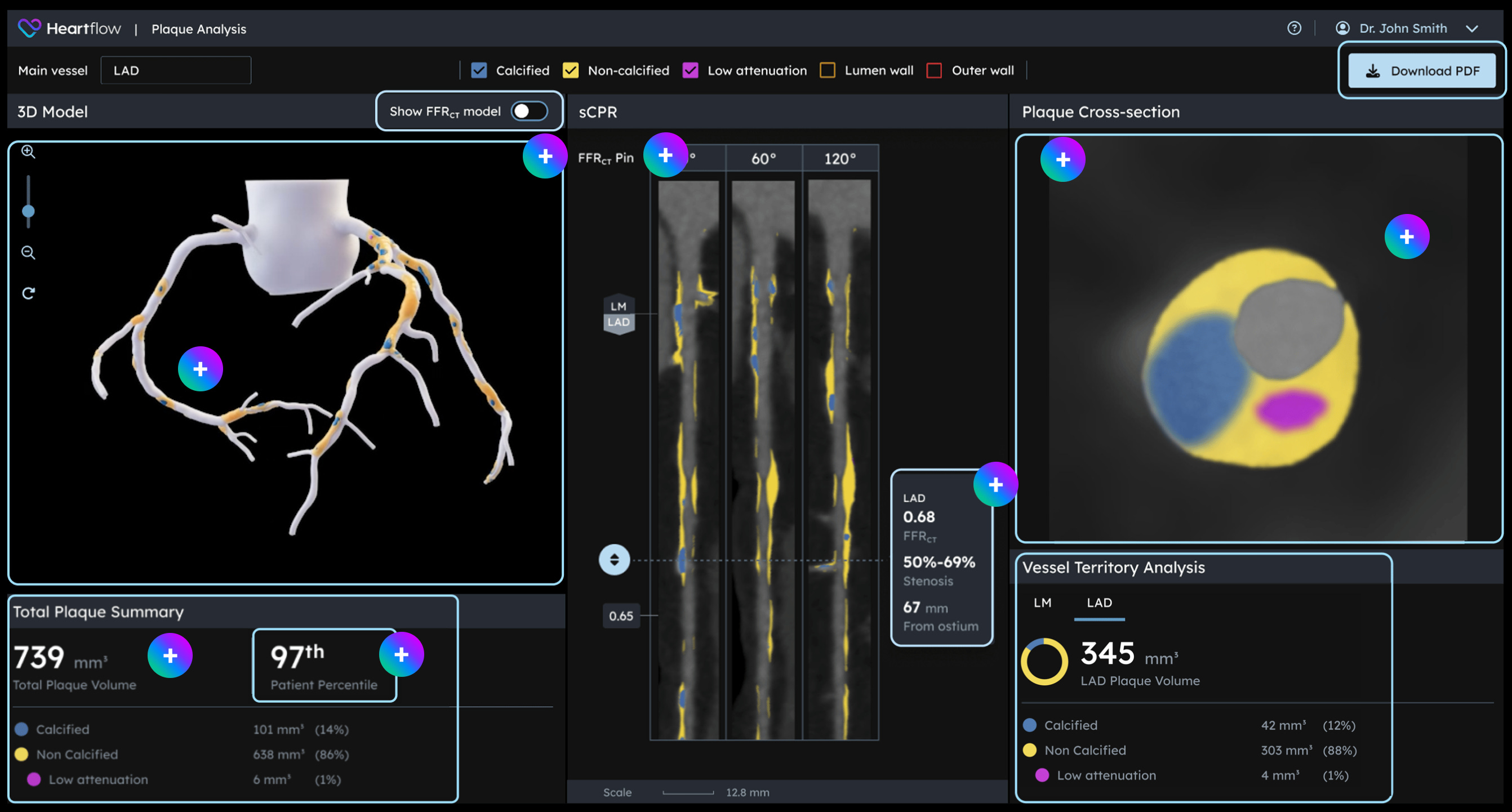
A standard CCTA read can tell us about stenosis, plaque, and anatomy. But AI-assisted quantitative plaque analysis can go further. Platforms like Heartflow and Cleerly-style AI-QCT can quantify total plaque volume, non-calcified plaque volume, low-attenuation plaque, and percent atheroma volume across the coronary tree.
That matters because plaque burden is not always obvious on a quick visual read, and because non-calcified plaque volume appears to carry prognostic information.
In the CERTAIN study, AI-QCT changed diagnosis or management in 57.1% of patients, reduced downstream testing by 37.1%, and increased preventive medication decisions compared with conventional CCTA interpretation alone.
In the CONFIRM2 registry, which followed 3,551 clinically indicated CCTA patients for a median of 4.27 years, non-calcified plaque volume and stenosis severity were independent predictors of major adverse cardiovascular events. Adding AI-QCT improved risk prediction beyond clinical models.
That is the Cleerly-type side of the story: what plaque is there, how much, and what kind?
HeartFlow and FFR-CT answer a different question: is a stenosis physiologically limiting blood flow? If CCTA shows an intermediate narrowing where anatomy alone does not settle the question, FFR-CT can help determine whether that lesion is causing vessel-specific ischemia and guide decision-making. NICE has also supported HeartFlow FFR-CT in selected patients with stable recent-onset chest pain who are already being offered CCTA.
Cleerly results and data on plaque categorization (cc: https://cleerlyhealth.com/what-is-cleerly)
Cardiac MRI belongs in this same functional lane. It is not the best tool for counting coronary plaque, but stress CMR is guideline-supported for diagnosing ischemia and estimating risk in intermediate-risk chest pain. It also adds tissue characterization: scar, myocarditis, cardiomyopathy, viability, and in some centers microvascular assessment.
These tools answer different questions. Cleerly-style AI-QCT is about plaque burden and plaque composition. HeartFlow-style FFR-CT and stress CMR are about physiology, ischemia, and downstream myocardial effects.
In the right patient, they are complementary. One tells us what is in the wall. The other tells us what it is doing to flow.
For South Asians, that combination may become particularly valuable because atherosclerosis can be earlier, quieter, and easier to miss before it becomes obviously obstructive.
How to Think About the Decision
Here is the practical way to think about it and organizing when CAC or CCTA might be an option.
Continue reading this post for free, courtesy of Omar Saleem, MD.